An extrasystole is an early heartbeat that comes before its turn. People often describe this as “my heart skipped a beat” or “my heart did a flip.” In medicine, the term used is premature beat. So extrasystole, premature beat, and what people call a “skipped beat” are all the same thing.
A healthy heart beats in a steady pattern. This pattern is set by the heart’s own electrical system. Signals come in order, and the heart contracts evenly. In an extrasystole, an extra signal comes from a different part of the heart out of turn, and the heart beats once before it should.
After this early beat, the heart waits a short while to get back into rhythm. This short pause is what makes the patient feel “my heart stopped for a moment.” The next normal beat that follows feels stronger because the heart had more time to fill with blood during the pause. So patients often say “it stops, then thumps.” In reality, the heart does not stop; only the timing of one beat has shifted.
Types of extrasystoles
Extrasystoles fall into two groups based on where in the heart they come from.
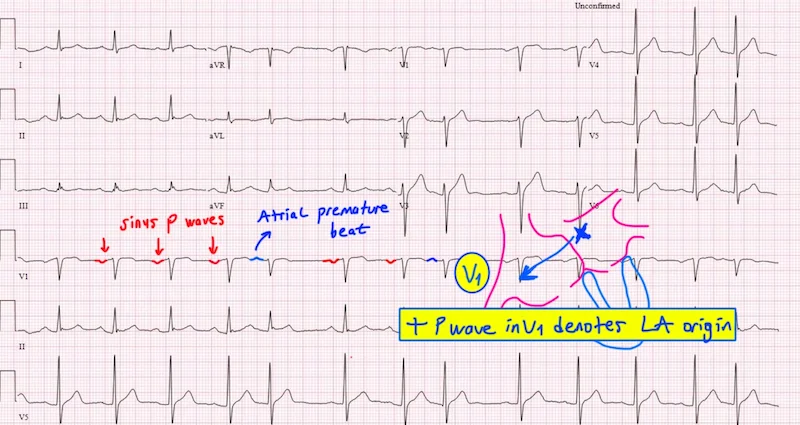
PAC (premature atrial contraction), also called SVES, is an early beat that starts in the upper chambers of the heart. The upper chambers are the small spaces where blood first enters the heart. An early signal from here usually stays quieter, and many patients do not notice it.
PVC (premature ventricular contraction), also called VES, is an early beat that starts in the lower chambers. The lower chambers are the larger spaces that pump blood out to the body. An early beat from here is felt more strongly. Most patients describe this type. The “felt” extrasystoles are mostly PVCs.
The difference between the two is shown on an ECG. An ECG, also called an EKG, is a simple, painless test that turns the heart’s electrical activity into a recording. This recording shows where the early beat came from.
What causes them?
Extrasystoles are very common. Most healthy people have a few each day; usually they are not even noticed. So having an extrasystole does not mean the heart is unwell.
Some things make early beats happen more often. Caffeine, tea, chocolate, alcohol, and smoking are leading triggers. Lack of sleep, fatigue, stress, and excitement also make the heart’s electrical system more sensitive. An overactive thyroid, anemia, and electrolyte imbalances (especially low potassium and magnesium in the blood) can lead to early beats. Some medications cause extrasystoles as a side effect.
Early beats can also show up without any of these. Some people have a slightly more sensitive electrical system from birth, and extrasystoles appear without a clear reason. This can last a lifetime but is usually harmless.
In people with a known heart condition, the frequency and meaning of extrasystoles are looked at differently. If there is a history of heart attack, heart failure, or a heart muscle disease, early beats are reviewed more carefully.
What are the symptoms?
Many people have no idea they have extrasystoles. The condition is found by chance during a routine ECG or Holter recording.
In those who do feel them, the most common complaint is “my heart skips a beat,” “it pauses, then beats hard,” or “I feel a catch in my chest.” Some patients describe it as an urge to cough, a slight tightness in the throat, or an uncomfortable feeling in the chest.
Early beats are usually felt more clearly during rest, especially when lying down or in quiet surroundings. The reason is that the body relaxes and awareness of the heartbeat goes up. The same beats may go unnoticed during activity through the day.
If extrasystoles come along with dizziness, near-fainting, shortness of breath, or chest pain, the situation is looked at differently. These symptoms point to something beyond a simple extrasystole.
Are they dangerous?
The vast majority of extrasystoles are harmless and not life-threatening. They do not wear out the heart, shorten life, or lead to a heart attack. So saying “I have extrasystoles” alone does not point to danger.
But two situations call for closer attention. The first is when the number of early beats is very high. People with more than 10,000 PVCs a day may, over many years, see the heart’s pumping power weaken. So high-count PVCs are followed regularly and treated when needed. The second is when the person has a known heart condition. Extrasystoles on the ground of a previous heart attack or heart failure are taken more seriously.
This is why there is no single answer to “is it dangerous?” The number, type, and the person’s heart structure are reviewed together.
How are they diagnosed?
The main tools used for diagnosis are an ECG and a Holter monitor. An ECG is a short recording; it only shows beats during the moment it is taken. If the early beats are infrequent, they may not be caught on the ECG.
This is why a Holter is more important when looking at extrasystoles. A Holter is a small portable device worn for 24 to 48 hours that records every heartbeat. The patient takes it home and goes about daily life. After the recording, the total number of extrasystoles within all the beats is counted. This number is one of the key pieces of information that guides treatment.
In some cases, an echocardiogram is also done. An echocardiogram is an imaging test that uses sound waves to show the structure of the heart. This test shows whether the heart is structurally sound. Blood tests check thyroid hormones, anemia, and electrolyte levels.
What do the numbers mean?
Holter reports show numbers like “200 PVCs per day” or “12,000 PVCs per day.” These numbers often worry patients. But what the numbers mean depends on the type and the person.
As a general approach, having extrasystoles below 1% of total daily beats (roughly under 1,000 a day) is seen as low burden. Between 1% and 10% is seen as moderate, and above 10% is seen as high burden. High-burden PVCs need special follow-up and treatment when needed.
These cut-offs are not the whole picture on their own. The patient’s symptoms, heart structure, and other conditions are reviewed together. So the same number can mean nothing in one person and call for treatment in another.
Treatment approach
Extrasystoles that cause no symptoms and are few in number do not need treatment. Cutting back on triggers like caffeine, alcohol, and lack of sleep often brings clear relief. Even just being told that the situation is harmless is reassuring on its own; because what often bothers patients is not the extrasystole itself, but the worry it causes.
For extrasystoles that cause symptoms or affect daily life, medication can be considered. Beta blockers are the most commonly used. Beta blockers calm the heart’s electrical system and reduce how often early beats happen. If symptoms continue despite medication or beta blockers are not suitable, other rhythm-controlling drugs can be tried.
For PVCs that come in very high numbers and start to affect the heart’s pumping power, catheter ablation can be offered. Ablation is a procedure where the small area causing the early beat is silenced with energy. A thin catheter is passed through a vein up to the heart. The spot sending the early signal is mapped, and a short burst of energy taking the area out of action. PVC ablation has a high success rate in experienced hands.
If there is an underlying condition, that is dealt with first. Thyroid problems are managed. Anemia is corrected. Electrolyte imbalances are fixed. These steps alone often bring the number of extrasystoles down clearly.
Lifestyle tips
Coffee, tea, energy drinks, and cola — products with caffeine — are clear triggers in many patients. Cutting these back or stopping for a while brings a noticeable drop. Alcohol and smoking raise early beats in the same way.
A steady sleep routine matters. Many patients say their extrasystoles get worse after a sleepless night. Regular and enough sleep helps the heart’s electrical system stay more balanced.
Stress management is another key topic. Early beats are known to rise during periods of heavy stress. Regular walks, breathing exercises, and relaxation methods help here.
Regular, moderate exercise reduces extrasystoles in most patients. But very heavy exercise can be a trigger in some. The right type and intensity of a sports routine should be decided with a doctor’s input.
When to call the doctor
For someone already known to have extrasystoles, a clear rise in symptoms, or new dizziness, near-fainting, shortness of breath, or chest pain, calls for review. If what was an occasional skipped beat turns into long, intense periods that disrupt daily life, that also needs to be looked at.
For people with a known heart condition, any new extrasystole complaint should not be taken lightly. People with a family history of sudden death at a young age should also have their extrasystoles looked at carefully.
Frequently Asked Questions
My Holter report says 8,000 PVCs a day. Is that a lot?
That number is close to the moderate-burden range and does not lead to a decision on its own. Your symptoms, the structure of your heart, and any other conditions are reviewed together. The same number can mean different things in two different people.
Are extrasystoles normal during pregnancy?
The heart works harder during pregnancy, and extrasystoles can be felt more often. Most of the time they are harmless. Still, new or strong symptoms should be shared with the doctor.
Will ablation get rid of extrasystoles for good?
For PVCs coming from a single spot, ablation gives a lasting solution with a high success rate. When the source is from multiple spots or is widespread, success is more limited. Your doctor will share the result expected for your specific case.
Does the (my heart stopped) feeling really mean my heart stopped?
No. The feeling is misleading. After an early beat, the heart waits briefly, and the next beat comes through more strongly. That is why people say (it stops, then thumps.) The heart does not actually stop; only the timing of a beat shifts.