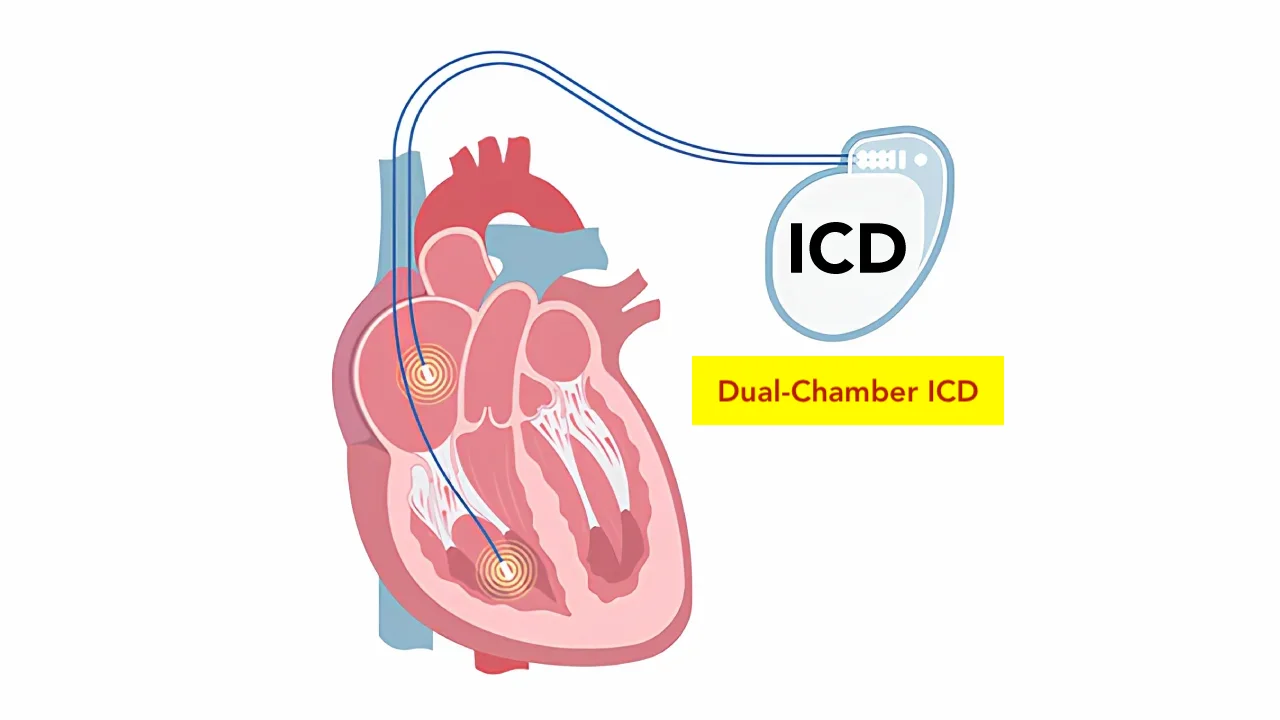
An implantable cardioverter defibrillator, or ICD for short, is a device that detects life-threatening rhythm disorders and steps in instantly. It is placed under the skin below the collarbone. The device does its job quietly; most of the time, the patient is not even aware it is there. But when a dangerous situation develops in the heart, it kicks in and carries out a protective action within seconds.
The main purpose of an ICD is to prevent sudden cardiac death. Sudden cardiac death is when the heart cannot pump effectively due to very fast and chaotic rhythm disorders coming from the lower chambers. This situation can be fatal within minutes. The moment an ICD detects such a rhythm, it acts on the heart to bring back the normal beat.
Are a pacemaker and an ICD the same thing?
This is a very important question because the two devices look similar from the outside but have different jobs. A pacemaker steps in when the heart beats too slowly and keeps the heart at a sufficient rate. An ICD deals with the opposite situation: it steps in when the heart is beating dangerously fast or working unevenly.
A pacemaker is a gentle helper; it is not a replacement for the heart but a device that lends support when needed. An ICD is a lifesaver; it stops the dangerous rhythm and brings back the normal beat. Most ICDs actually carry out the function of a pacemaker as well; that is, they correct slowness when needed and end dangerous fast beats when needed.
The most clear difference between them is what the device can do. A pacemaker only sends small electrical signals. An ICD, on top of these signals, can deliver a high-energy shock when needed. This is where the “shock” feature, which patients are most curious about, comes in.
Who gets an ICD?
The decision to place an ICD is made after a careful evaluation. Which patient gets one is decided based on the type of disease, the heart’s pumping power, and past rhythm events.
There are two main reasons for placement. The first is called secondary prevention. ICDs are placed in patients who have already had a dangerous rhythm disorder, survived a cardiac arrest, or had ongoing ventricular tachycardia (a fast heartbeat condition starting in the lower chambers of the heart). For these people, the risk of going through such an event again is high, and the device serves as a guard.
The second group is called primary prevention. These are patients who have not yet had a dangerous rhythm disorder but are at high risk. Those whose pumping power is clearly reduced after a heart attack, those with advanced heart failure, and those with certain inherited heart conditions (such as long QT syndrome, Brugada syndrome, hypertrophic cardiomyopathy) are in this group. Protection is provided in these patients before an event happens.
In inherited rhythm disorders such as Brugada syndrome, an ICD is of vital importance especially in high-risk patients.
The decision is always individual. Two patients with the same diagnosis may not both be ICD candidates. The doctor carries out the risk assessment with an echocardiogram (an imaging test that uses sound waves to show the structure of the heart), ECG, Holter, and an electrophysiology study when needed.
How does the device work?
An ICD constantly tracks the heart’s electrical activity. The software inside the device checks every beat, deciding within seconds whether the rhythm is steady or dangerous. So an ICD is, in a sense, a night watchman on duty 24 hours a day.
When the device detects a rhythm disorder, it picks one of three different actions.
The first is low-energy fast pacing. This is called anti-tachycardia pacing. The device sends very fast but low-power signals to the heart to break the fast rhythm. If this approach works, the patient feels nothing or only a mild fluttering. In most patients, the dangerous rhythm is ended this way.
The second is a synchronized shock. This is a stronger shock delivered with a specific timing. It is used for faster and more uneven rhythms.
The third is a full shock. It is delivered for the most dangerous rhythm disorders such as ventricular fibrillation. This high-energy shock briefly resets all the heart’s electrical activity; after the reset, the heart catches its own normal rhythm. This is the lifesaving shock.
The software decides which action to take; this software is set up specifically for each patient. The whole process is completed within seconds.
How is the device placed?
The procedure is done in an operating room but it is not considered major surgery. The patient is not put fully to sleep; only the area below the collarbone is numbed. So no pain is felt. A mild sedative can also be given based on the patient’s preference and the situation.
A small cut is made in the skin and a pocket is created where the device will sit. The wires from the device are guided through a vein near the collarbone and into the heart. Imaging is used to make sure the wires are in the right place. The device is then placed under the skin and the cut is closed with stitches.
The procedure usually takes one to two hours. During the procedure, a controlled test may be done to make sure the device works correctly. During this test, the patient is put to sleep and it is checked whether the device gives the right response under real conditions.
Most patients go home the next day. For the first few days, care should be taken with arm movements; the arm on the side of the device should not be lifted above shoulder height. This keeps the wires from shifting.
What does a shock feel like?
This is what patients wonder about most. How a shock feels depends largely on whether the patient is conscious at that moment.
If the patient has lost consciousness due to the dangerous rhythm disorder, they do not feel the shock being delivered. When they come around, they wake with the feeling that “something happened.”
For a conscious patient, the shock feels different. Most patients describe it as “a horse kicked me in the chest” or “a sudden punch.” It is a sharp but brief feeling that lasts less than a second. After the shock passes, a slight chill and mild chest soreness usually remain.
A shock can be frightening; this is a perfectly natural response. But the purpose of a shock is to save life. A shock from an ICD shows that the patient’s life was in danger at that moment and that the device did its job.
Some patients develop a fear of shocks after the device is placed. To deal with this feeling, talking openly with the doctor and getting psychological support when needed is helpful. Support groups for people with ICDs can also be useful.
What should I do when I get a shock?
If your device delivered a shock, there is a simple roadmap to follow.
The moment you get a shock, sit or lie down in a safe place first. If you are alone and feel unwell, ask someone for help immediately.
If you feel fine after the shock and have no other symptoms, getting a single shock is often not an emergency. But you need to reach your doctor on the same day. Most centers have a 24/7 line for ICD patients.
If you got more than one shock back-to-back, go to the emergency room or call an ambulance. This means the device is dealing with a problem and needs prompt evaluation.
If fainting, dizziness, chest pain, or shortness of breath comes after the shock, these call for emergency evaluation.
When going to the doctor, carry the card or records with information about the device’s brand, model, and follow-up center. This information speeds up the evaluation process.
Living with the device
Most patients return to their normal lives after getting an ICD. In the first weeks, mild tenderness and some swelling at the site are normal; this is expected and settles with time. Once the skin heals, the device feels like a small bump under the skin from the outside.
There are some things to be careful about in daily life. Mobile phones are safe to use; just avoid carrying the phone in the chest pocket on the same side as the device. During calls, holding the phone to the opposite ear instead of close to the device is the right way.
Microwaves, televisions, computers, hair dryers, and other household appliances do not cause problems. There is no need to fear the appliances you use in the kitchen and daily life.
Airport security gates can be passed through, but the staff should be told about the ICD, and a hand search is preferred. Walking through quickly usually causes no problem; but standing near the gate for a long time should be avoided.
Some medical devices and situations should be avoided. Devices that create strong magnetic fields (older type MRI machines), electrosurgery (the electrical cutting tool used in some surgeries), some physical therapy methods, and TENS devices used for pain relief may not be compatible with an ICD. Always tell about your device before any medical procedure.
The situation around MRI is changing. With older devices, MRI was not safe. Most newer ICDs are MRI-compatible. Before the scan, the brand and model of the device should be shared, and both the MRI center and the cardiology team should be informed.
Going through theft alarms, store security gates, and metal detectors quickly usually causes no problem. For industrial magnetic fields (large generators, transformers, welding machines), you should consult your doctor about the safety rules at your workplace.
Driving and work life
One of the most common questions among ICD patients is about driving. There are restrictions here; because in case of a possible shock or fainting while at the wheel, it puts both you and those around you at risk.
For patients who got an ICD for secondary prevention (those who already had a rhythm event), driving restrictions are stricter. Generally, no driving is advised for the first three to six months. After this period, driving permission is given with a doctor’s evaluation.
For patients who got an ICD for primary prevention (those who have not had an event yet), the restriction is shorter; private vehicle use is usually considered safe a few weeks later.
Commercial vehicle (bus, truck, taxi) use is not allowed for ICD patients in most countries. The rules on this vary by regulation; current regulations should always be checked.
In work life, most jobs can be continued without problems with an ICD. But working with high-voltage electrical tools, professional welding, and working in environments with large industrial magnetic fields call for evaluation. Some specific jobs such as pilot or diver generally cannot be done with an ICD.
Sports and physical activity
Most patients who get an ICD can do sports. Walking, swimming (the device is waterproof), cycling, and light exercise are safe.
But sports where there is a chance of taking a direct hit to the chest area (boxing, martial arts, contact in football, basketball, and so on) are not advised because they can damage the device. Sports that involve lifting weights with the arm on the device side (such as bodybuilding) can also strain the wires; for this reason, they are not suitable.
A separate evaluation is needed for competitive sports. Very high-intensity competitive sports can both strain the heart and trigger a rhythm disorder, and a possible shock during a competition could be dangerous.
Battery life and check-ups
The battery inside the ICD lasts for years. Most modern devices have a battery life between five and ten years. This time varies based on how often the device steps in and which type of signals it uses. Devices that constantly act as a pacemaker or deliver frequent shocks wear down the battery faster.
When the battery runs out, only the battery part of the device is replaced, not the whole device. This procedure is not as difficult as the first placement; because the wires are already in place, only the pocket is reopened and the device is swapped. The second procedure is usually shorter.
Regular check-ups are needed to make sure the device is working as it should. Check-ups are usually done every three to six months. During these check-ups, a special device reads the ICD’s battery, wires, detected events, and delivered actions. Even when a patient thinks they have never had a shock, the device records events that may have happened in the background; check-ups are important for seeing these records.
Many newer devices have remote monitoring. The patient is given a receiver; this receiver is kept in the bedroom and regularly sends device data to the doctor. So if a problem comes up between check-ups, it is noticed quickly.
Frequently Asked Questions
How will my life change after getting an ICD?
Most patients continue with their normal lives. Apart from some restrictions to keep in mind for the first few weeks, quality of life is largely preserved in the long run. On the contrary, an ICD reduces the worry of sudden cardiac death in high-risk patients, which improves quality of life.
Is getting a shock very painful?
A shock received while conscious is a sharp but brief feeling. It is described with phrases like "a kick to my chest." It is painful but lasts less than a second and saves life. A shock received while unconscious is not felt.
Can the device deliver a shock by mistake?
It can rarely happen. During very intense exercise, the device may mistake the heart rate for a dangerous rhythm, or wrong signals from the wires can lead to such situations. The device's programming is set to keep these wrong shocks to a minimum. If you think you got a wrong shock, you should reach the doctor; the device settings can be reviewed.
Will my sex life be affected?
No. An ICD does not get in the way of a sex life. The normal rise in heart rate during sexual activity is not seen as a problem by the device. What matters is feeling at ease.
Can I fly after getting an ICD?
Yes. Flying does not affect the device. At airport security, telling the staff and asking for a hand search is enough. Carrying your ICD card makes things smoother.
Can I have an MRI?
Most newer devices are MRI-compatible. Before the scan, the brand and model of the device should be shared, and both the MRI center and the cardiology team should be informed. The situation may be different for older devices.
Will my medications be stopped after getting an ICD?
For most patients, medications continue. An ICD is a guard; it does not replace the medications that prevent rhythm disorders or treat heart failure. Rhythm medications, beta blockers, and heart failure medications usually continue as before.
If the device delivers a shock while my family is near me, will it harm them?
No. Someone touching you when the device delivers a shock may feel a very mild tingling, but it is not harmful. There is no need to fear close contact with your spouse or child.
I am afraid of getting an ICD. Is this normal?
This is a perfectly natural response. The idea of having a new device placed in the body, the concept of "shock," and the worry that life will change make many patients afraid. Do not hesitate to share these feelings with your doctor. Most centers offer counseling for ICD candidates and provide the chance to talk with patients who already have an ICD. The fears often pass through knowing.