Atrial fibrillation ablation is a treatment aimed at correcting the disorganized rhythm that arises in the upper chambers of the heart. The goal of the procedure is to stop the faulty signals that start atrial fibrillation from spreading to the heart and to bring the heart back to its steady beat.
Atrial fibrillation (AFib) is a condition in which the upper chambers of the heart contract in a fast and disorganized way. The upper chambers are called the atria. The atrium is the chamber where blood first collects in the heart. In a healthy heart, the atria contract in a steady rhythm and pass the blood on to the lower chambers. In AF, this order breaks down; the atria contract in a quivering manner, and the heart beats both fast and unevenly.
Most of these faulty signals come from the area where the veins carrying blood from the lungs meet the heart. These veins are called the pulmonary veins. The pulmonary veins are the four main veins that carry oxygen-rich blood from the lungs to the heart. In some people, the cells where the atrium meets these veins start sending faulty electrical signals and bombard the atrium. The basis of AF ablation is to build a kind of “electrical wall” around these veins so the faulty signals cannot pass into the atrium. This is called pulmonary vein isolation.
Who is this procedure for?
Not every patient with AF is offered ablation. Whether the procedure is the right step depends on the type of AF, how often it happens, the response to medication, and the patient’s overall health.
For patients who keep having AF episodes despite medication and whose daily life is affected, ablation is the strongest option. Rhythm-controlling drugs often reduce the number of episodes but are not enough in some patients; in these people, ablation brings clear relief. Patients who have side effects from medication are also good candidates for ablation.
Even in newly diagnosed AF, ablation may be offered early in some cases. In younger patients, when AF has not yet affected the heart’s structure, the success rate of early ablation is higher. Recent studies have shown that ablation done early on gives better long-term results.
But ablation is not the first choice for every patient. If AF has become continuous over the years, if the upper chambers have widened clearly, or if there are advanced structural problems in the heart, the success rate drops. A different treatment plan is considered for these patients.
How is it done?
AF ablation is done through the blood vessels. So the chest is not opened, and it is not considered open-heart surgery. The patient is put to sleep or placed under deep sedation. Sedation is the use of medication that takes the patient into a painless and comfortable sleep-like state without full anesthesia. The choice of method varies by center.
The procedure starts at the large vein in the groin. Thin catheters are advanced from this vein up to the heart. A catheter is a thin, flexible tube that delivers energy or carries out mapping from its tip. To reach the left side of the atrium, a thin wall between the two upper chambers is carefully crossed. This step is called transseptal access.
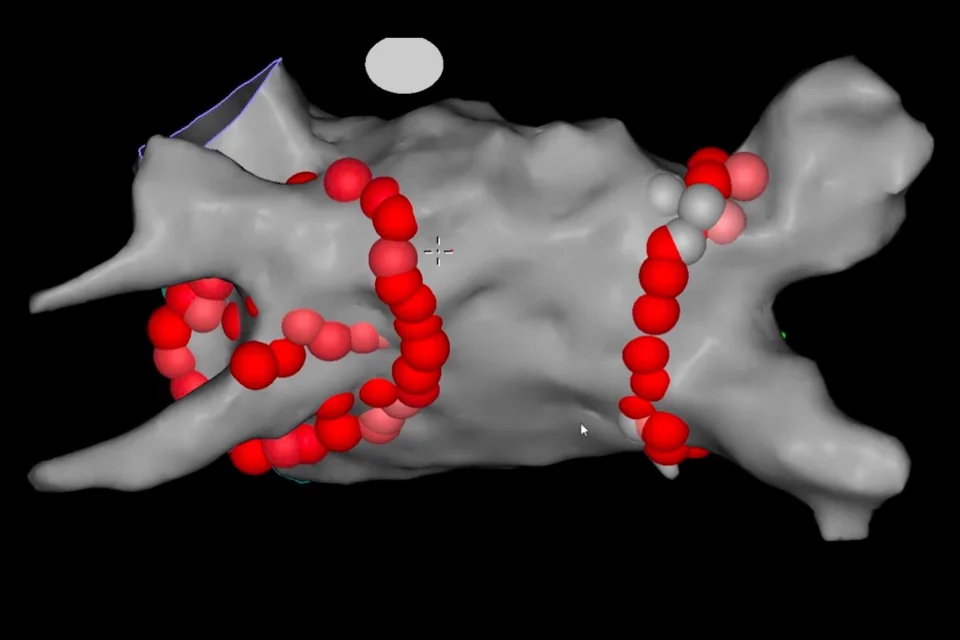
Once the left atrium is reached, a map is created first. Modern systems display a real-time three-dimensional view of the atrium on the screen. The doctor sees clearly where the pulmonary veins meet the atrium. Starting from these points, the team works around each vein, and short bursts of energy take small areas of tissue out of action. When a closed ring is created around the veins, faulty signals from the pulmonary veins can no longer pass into the atrium.
The procedure usually takes between two and four hours, depending on the type used.
What kind of energy is used?
Three different types of energy can be used in AF ablation.
Radiofrequency ablation uses heat. A high-frequency electrical current delivered from the catheter tip warms the tissue and shuts down the faulty signal path. This method has been in use for decades and offers wide experience.
Cryoablation uses cold. A balloon at the catheter tip is placed at the opening of the pulmonary vein and inflated. A cooling gas is sent into the balloon; the balloon freezes and takes a small area of the surrounding tissue out of action. Cryoablation is a particularly suitable approach for AF because each of the four pulmonary veins can be treated one by one with the balloon. Its procedure time can be shorter than with radiofrequency.
Pulsed field ablation (PFA) is a newer method introduced in recent years. In this approach, very short bursts of high-voltage electricity are sent to the tissue. The most important feature of PFA is that it works selectively; it only affects heart tissue and does not harm nearby structures such as the esophagus, nerves, or blood vessels. This feature makes the procedure safer and is seen as a major step forward in treatment.
The choice of energy depends on the patient, the type of AF, the structure of the heart, and the experience of the center. The success rates of all three methods are close to each other; the choice between them is largely based on procedure time, safety profile, and suitability.
A clear word about risks
Like any procedure, AF ablation carries risks. In experienced hands, serious problems are rare but not zero. It is important that the patient is informed about this.
Bruising and bleeding at the groin entry site are among the most common issues. They are usually small and clear up in a few days. Less commonly, fluid can collect in the sac around the heart; this is called pericardial effusion. In most cases, it is noticed during the procedure and dealt with in the same session.
Narrowing of the pulmonary veins over time is a very rare complication. Because the esophagus sits close to the left atrium, heat-based methods can rarely cause problems in the esophagus. PFA has a safer profile in this regard. The risk of stroke is very low at experienced centers; the use of blood thinners during the procedure keeps this risk to a minimum.
Which risks come into play depends on the type of procedure, the patient, and the center’s experience. So before the procedure, the doctor should inform the patient about the risks specific to their situation in detail.
After the procedure
When the procedure ends, the patient is followed in the recovery area for a few hours. Pressure is applied to the entry site at the groin, and the patient is asked to lie still for several hours. This is to prevent bleeding. Most patients are sent home the same day or after one night.
Tenderness and mild bruising at the entry site are normal in the first few days. During this time, heavy lifting and demanding sports should be avoided. Walking and light daily activity can be started after a few days. Most patients return to work within a week.
The first three months after the procedure are a special period. This is called the “blanking period.” During this time, the treated area heals and the tissues in the atrium settle. Palpitations may come back during this period, but this does not mean the ablation has failed. The assessment done at the end of three months shows the real result.
Blood thinners continue for at least three months; this period is to reduce the risk of clot formation after the procedure. After three months, the decision to continue the medication is based on the patient’s stroke risk score. This score is calculated by looking at the patient’s age, other medical conditions, and other factors.
Rhythm-controlling medications may also continue for a while after the procedure. The doctor checks the heart rhythm at the end of the blanking period and decides on reducing or stopping the medications.
How lasting are the results?
The success rate of AF ablation depends on the type of the disease. In paroxysmal AF, where episodes come in attacks and stop on their own, the success rate is high. After a single session, 70-80% of patients achieve long-term rhythm control. In persistent AF, the success rate is somewhat lower; some patients may need a second ablation session.
When the result is not lasting, the reason is usually that the electrical wall created during the ablation starts allowing signals through at some points over time. In a second procedure, these leaking points are found and closed.
Ablation alone is not enough for AF to stay away in the long run. Weight control, management of high blood pressure and diabetes, cutting back on alcohol, treating sleep apnea, and regular exercise are key factors that make ablation success last. Without lifestyle changes, the recurrence rate is higher.
Frequently Asked Questions
Does ablation cure AFib completely?
For some patients yes, for some only partly. In paroxysmal AFib, the chance of long-term improvement after a single session is high. In persistent AFib, full improvement is less common; in some patients episodes are reduced but may not go away completely. Your doctor will share the result expected for your specific case.
Are blood thinners stopped after the procedure?
Blood thinners are required for at least the first three months. After three months, whether to continue depends on the patients stroke risk score. In low-risk patients, they may be stopped, while in high-risk patients, blood thinners continue for a long time even if the ablation is successful. This is because AF can briefly come back even when no symptoms are felt.
Can I just stay on medication instead of ablation?
You can, but it may not be enough for every patient. Medications often reduce how often episodes happen but do not fully remove AFib. For patients with side effects, frequent episodes despite medication, or those who want a more lasting rhythm control, ablation offers a clear advantage.
If one ablation is not enough, how many can be done?
A second or even a third session can be done if needed. The success rate after a second session is usually higher because the leaking points from the first procedure are found and closed.
Can I return to normal life right after the procedure?
Most patients return to work and daily life within a week. For demanding sports and heavy physical activity, two weeks of rest is advised. Walking and light activity can be started within a few days.
Which is better; cryoablation, radiofrequency, or PFA?
The success rates of all three methods are close. Which one is suitable depends on the patients anatomy, the type of AFib, and the experience of the center. What matters is that the procedure is done with the right method by an experienced team.
Is ablation a painful procedure?
The patient is put to sleep or placed under deep sedation, so no pain is felt during the procedure. Mild tenderness may continue at the groin entry site for a few days; simple pain relievers ease it.
How long does follow-up last after the procedure?
Close follow-up is done for the first three months. After that, a check-up every six to twelve months is usually enough. ECG is taken during follow-up, and a Holter is added when needed. A Holter is a small portable device worn for 24 to 48 hours that records every heartbeat.