Ablation is a procedure that offers a lasting treatment for rhythm disorders of the heart. The aim of the procedure is to take the source or pathway of the faulty signals (which cause the heart to beat unevenly, too fast, or too slow) out of action. This way, the heart returns to its steady rhythm.
The word ablation is often understood by the public as “burning.” This creates a wrong impression. The heart is not burned during the procedure; controlled energy is applied to a very small tissue area (usually a few millimeters in size) that is causing the problem. This energy stops that point from conducting electricity. The rest of the heart is not affected in any way. The procedure is a highly focused and precise treatment.
A healthy heart beats steadily through its own electrical system. This system spreads from the upper chambers throughout the heart with each signal. In some people, glitches develop in this system: an unwanted shortcut may be present, an extra spot may produce faulty signals, or the electrical current may go around in a loop. These glitches lead to rhythm disorders. Ablation is a treatment that finds the exact location of the glitch and takes care of the problem there.
What conditions is ablation used for?
Ablation is used for a wide range of rhythm disorders. The most common condition treated with ablation is supraventricular tachycardia. For this fast palpitation that comes in episodes, starting and stopping suddenly, ablation offers a lasting solution with a very high success rate.
Ablation is also at the forefront for patients with Wolff Parkinson White (WPW) syndrome, who have palpitation episodes due to an extra electrical pathway present from birth. In this case, the extra pathway is closed off with the procedure, and the patient may never have another palpitation episode.
In atrial fibrillation, ablation is done with a different approach. Instead of silencing a single point, an electrical wall is built around the pulmonary veins in the upper chamber of the heart. This wall stops faulty signals from passing into the atrium. Details are covered in the atrial fibrillation ablation article.
For frequent premature beats (extrasystoles), ablation is used especially for those that come in high numbers and from a single spot. In atrial flutter, a regular fast rhythm disorder similar to atrial fibrillation, ablation also offers a lasting solution. Ventricular tachycardia, a fast heartbeat that starts in the lower chambers, is another condition where ablation is an important treatment option.
The decision on which condition will be treated with ablation is made based on the patient’s symptoms, the type of rhythm disorder, the response to medication, and other accompanying conditions.
How is ablation done?
Ablation is done through the blood vessels. So the chest is not opened, and it is not considered open-heart surgery. The procedure is carried out in an operating room or in an electrophysiology laboratory. This laboratory is a space specially equipped for studying and treating the heart’s electrical system.
The type of anesthesia depends on the type of procedure. Some procedures are done under general anesthesia; the patient is fully put to sleep. Others use sedation. Sedation is the use of medication that takes the patient into a painless and comfortable sleep-like state without full anesthesia. The doctor decides which method is suitable.
The procedure starts at the large vein in the groin. The area is first numbed and a thin sheath is placed in the vein. Thin and flexible tubes are passed through this sheath. These tubes are called catheters. A catheter is a thin, flexible tube that delivers energy or carries out mapping from its tip. Several catheters can be used at the same time. The catheters are advanced through the vein up to the heart.
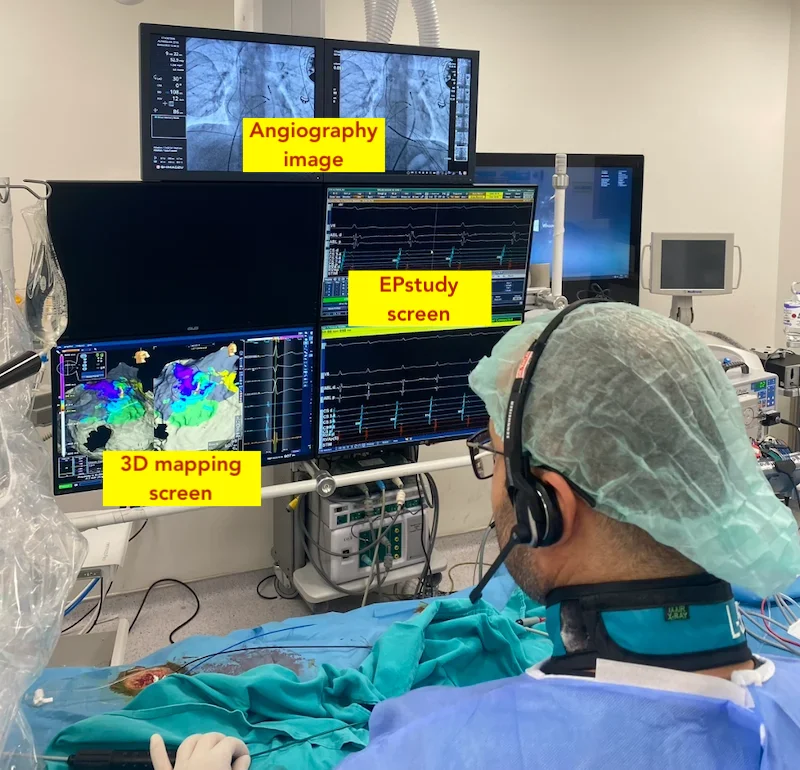
Once the heart is reached, the mapping stage begins. Modern systems display a real-time three-dimensional view of the heart on the screen. The doctor watches how the heart is working electrically through this map. The exact spot where the faulty signal is coming from or which pathway it is following is identified with millimetric precision.
Once the right spot is identified, the ablation step begins. Controlled energy is delivered from the catheter tip, and that small tissue area is taken out of action. To make sure the problem is solved, the heart is tested again after the procedure; the heart is stimulated to see whether the same rhythm disorder starts again. If it does not, the procedure is considered successful.
The procedure time varies by type and complexity. A simple supraventricular tachycardia ablation takes one to two hours, while atrial fibrillation or ventricular tachycardia ablation can take three to six hours.
What types of energy are used?
Different types of energy can be used in ablation. Which one is preferred depends on the type of ablation and the patient’s condition.
Radiofrequency energy (heat) is the most commonly used method. A high-frequency electrical current delivered from the catheter tip warms the tissue and shuts down the faulty signal pathway. This method has been in use for decades and offers wide experience.
Cryoablation (cold) is the preferred method in some cases. The tissue is frozen and taken out of action. It is widely used in atrial fibrillation ablation with special balloon-shaped catheters.
Pulsed field ablation (PFA) is a newer method introduced in recent years. Very short bursts of high-voltage electricity are sent to the tissue. The important feature of PFA is that it works selectively; it only affects heart tissue and does not harm nearby structures.
The choice of which energy type to use is made based on the type of disease, the structure of the heart, and the experience of the center. The success rates of all three methods are close to each other.
A clear word about risks
Ablation is a safe procedure in experienced hands. But like any medical procedure, it carries certain risks, and sharing them openly is the right approach.
Bruising and mild bleeding at the entry site in the groin are the most common findings. They usually clear up on their own. Less commonly, larger bleeding or vessel injury can occur.
Fluid collection in the sac around the heart (pericardial effusion) can develop in a small number of patients. This is noticed during the procedure and dealt with in the same session. In very rare cases, this fluid may call for urgent attention.
The risk of stroke is very low at experienced centers. The blood thinner treatment given during the procedure keeps this risk to a minimum. In ablations done in the left atrium, such as for atrial fibrillation, this risk is somewhat higher than in others.
In ablations done near the atrioventricular node, an important point of the heart’s electrical system, there is a risk of harm to this structure. This is rare, but if it happens, a permanent pacemaker may be needed. So ablations done near this area are planned with special care.
Risks vary by the type of procedure. In more complex procedures such as epicardial ablation, the risk profile is different, and these procedures are done at centers with special expertise.
Preparation before the procedure
Some preparation is needed before the procedure. The doctor usually asks for some rhythm-controlling medications to be stopped about a week before; this is so the rhythm disorder can be brought out during the ablation. For patients on blood thinners, how the medication will be managed is planned by the doctor.
Nothing should be eaten from the night before the procedure. Water intake is also stopped a few hours before. Which of the regularly used medications should be taken in the morning and which should not is informed by the doctor.
Routine blood tests and an ECG are done before the procedure. In some patients, an echocardiogram is also requested. An echocardiogram is a painless imaging test that uses sound waves to show the structure of the heart. For patients who will have an atrial fibrillation ablation, a special echocardiogram done through the esophagus (transesophageal echocardiogram) may be needed to make sure there is no clot inside the heart.
After the procedure
When the procedure ends, the patient is followed in the recovery area for a few hours. Pressure is applied to the entry site at the groin, and the patient is asked to lie still for several hours. This is to prevent bleeding. Most patients go home the same day or after one night. After complex ablations, the hospital stay may last one to two days.
Tenderness and mild bruising at the entry site are normal in the first few days. During this time, heavy lifting, squatting, and demanding sports should be avoided. Walking and light daily activity can be started a few days later. Most patients return to work within a week.
Some palpitations may occur in the early period after the procedure. The first three months after atrial fibrillation ablation are especially special in this respect; this period is called the “blanking period.” During this time, the treated area heals. Having palpitations does not mean the ablation has failed. In other ablation types as well, occasional palpitations may be felt for a few weeks after the procedure; these usually fade with time.
The doctor schedules follow-up visits. The first check-up is usually within one to two weeks. Later visits are at three, six, and twelve months. ECG is taken at follow-ups, and a Holter is added when needed. A Holter is a small portable device worn for 24 to 48 hours that records every heartbeat.
What happens with medications after the procedure varies by case. In some patients, rhythm medications can be stopped. In others, they continue at a low dose. In atrial fibrillation, blood thinners are used for at least three months; what comes after is decided based on the patient’s stroke risk score. Stopping medications on your own is not the right path; they are always adjusted with the doctor’s decision.
How is the success rate?
The success rate of ablation varies clearly by type.
In supraventricular tachycardia (AVNRT, AVRT, WPW), the success rate is very high (%95-98). After a single session, the problem is solved permanently in most patients.
In premature beat ablation, success varies based on whether the beats come from a single spot or multiple spots. In single-source cases, high success is achieved, while in widespread cases, results are somewhat more limited.
Atrial flutter ablation offers high success. In paroxysmal atrial fibrillation (the type that comes in episodes), 70-85% of patients achieve long-term rhythm control after a single session. In persistent atrial fibrillation, success is somewhat lower.
In ventricular tachycardia, success varies clearly based on the underlying condition. In ventricular tachycardia from a single spot in a healthy heart, high success is achieved. In patients with structural heart disease, the spots can be more widespread, and more than one session may be needed.
For patients who do not get a result after a single session, a second or even a third session can be done. The success rate after a second session is usually higher.
Frequently Asked Questions
Is ablation considered surgery?
No. Ablation is done through the blood vessels. The chest is not opened, and there is no open-heart surgery. The entry is just through a small puncture in the groin. The recovery is fast accordingly.
Will I feel pain during the procedure?
No. The patient does not feel pain because they are put to sleep or placed under deep sedation. Mild tenderness may continue at the entry site in the groin for a few days; simple pain relievers ease it.
Can the rhythm disorder come back after ablation?
It depends on the type. In conditions like supraventricular tachycardia and WPW, recurrence is very rare. In more complex rhythm disorders such as atrial fibrillation, the chance of recurrence over time is higher; a second procedure may be needed.
Can I stop my medications after ablation?
That decision belongs to your doctor. In some patients, medications can be stopped; in others, they continue at a low dose. Even when ablation is successful, blood thinners may continue for a long time in some patients; the reasons for this decision will be shared with you.
Does ablation harm the heart?
No. The heart is not harmed during ablation. Only a very small tissue area (usually a few millimeters) causing the problem is taken out of action. The rest of the heart continues to work normally. The pumping power of the heart is not affected.
Can ablation be done during pregnancy?
As much as possible, ablation is not done during pregnancy because the X-rays used during the procedure can pose a risk to the baby. For women planning pregnancy, ablation before conceiving is offered. In very urgent cases, it can be done during pregnancy with special precautions to protect the baby.
Can ablation be done at every hospital?
No. Ablation is done at centers with an electrophysiology laboratory and a team trained in this field. For complex ablations, the experience of the center directly affects the result.
Is fasting before the procedure required?
Yes. Nothing should be eaten from the night before the procedure. Otherwise, there is a risk of stomach contents passing into the lungs during anesthesia. Water intake is also stopped a few hours before the procedure.
When can I return to my normal life after ablation?
Most patients return to work and daily life within a week. For demanding sports and heavy physical activity, two weeks of rest is advised. Walking and light activity can be started within a few days.
Can I do sports after the procedure?
Yes. Most sports can be resumed once recovery is complete. If the ablation is successful, the restrictions placed because of the rhythm disorder can also be lifted. It is important to get the doctor's clearance about which sports you can return to and when.