Wolff-Parkinson-White syndrome is a arrhythmia caused by an extra electrical pathway that has been present in the heart since birth. This extra pathway can make the heart beat very fast at times. The condition takes its name from the three doctors who first described it together in 1930. Since then it has been known by their initials as WPW.
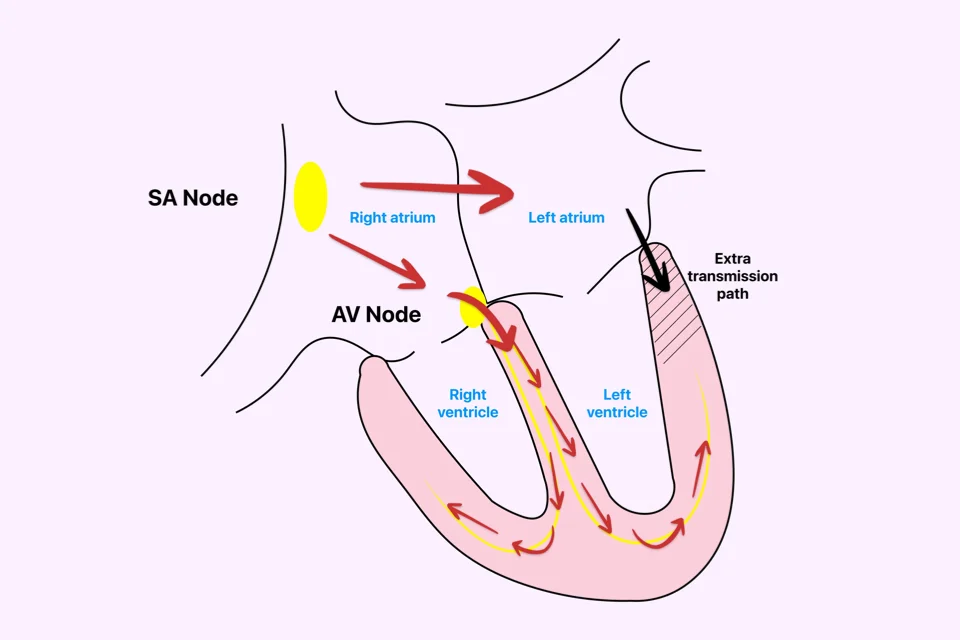
To understand the condition, it helps to start with how the heart normally works. Each heartbeat is set off by an electrical signal that begins in the upper chambers. As this signal moves down to the lower chambers, it pauses briefly at a relay point. This short pause lets the upper chambers fill the lower ones before the lower chambers push the blood out. A steady, useful beat depends on this pause.
In WPW, alongside this normal system there is also an extra shortcut, present from birth. When the signal travels down its usual path, part of it slips through this shortcut as well. The signal then reaches the lower chambers by two routes at once. A loop can form between these two paths, and this is what makes the heart suddenly race.
What are the symptoms?
Some people have no symptoms at all. The condition is picked up by chance on an ECG done for another reason. These people carry the extra pathway but have not had a racing episode yet.
In those who do have symptoms, the most common complaint is a fast heartbeat that comes on suddenly and stops just as suddenly. Patients often describe it as “my heart is going to jump out of my chest” or “it sped up out of nowhere and then just stopped.” An episode can last from a few minutes to a few hours.
Along with the fast heartbeat, there may be lightheadedness, weakness, a tight feeling in the chest, or shortness of breath. In rare cases, dimming of vision and fainting can occur. Symptoms usually begin in childhood or young adulthood. In some patients, episodes stay rare for years; in others, they grow more frequent over time.
Is it dangerous?
For most patients, WPW affects daily comfort but does not put life in danger. However, in a small group of patients (especially when WPW is accompanied by atrial fibrillation), the nature of the extra pathway can lead to a serious arrhythmia (a medical term for an abnormal heartbeat). This happens when very fast signals from the upper chambers race through the shortcut and reach the lower chambers far too quickly. The result can be a severe rhythm problem and, rarely, sudden cardiac arrest.
For this reason, every person found to have WPW is checked carefully to see how risky the extra pathway is. Athletes, people in physically demanding jobs, and those who have already had episodes are looked at most closely.
How is it diagnosed?
The first step is an ECG, also called an EKG. An ECG is a recording that shows the heart’s electrical activity on paper or a screen. WPW leaves a typical mark on this recording. An experienced doctor can often spot it at first glance.
But the extra pathway is not always active. The ECG can look normal at times and only show the pattern during a racing episode. So in patients with suspected episodes, a Holter monitor is often used. A Holter is a small portable device worn for one to several days that records every heartbeat. The patient goes about daily life while the device runs quietly in the background.
Once the diagnosis is clear, an electrophysiology study may follow. This is a procedure that takes a closer look at the heart’s electrical system. Thin wires are passed through a vein up to the heart, and the exact location and behavior of the extra pathway are mapped out. Treatment can be done in the same session.
Treatment options
Patients without symptoms do not always need treatment. If the risk looks low, regular follow-up may be enough. But if the patient is an athlete, has a physically demanding job, or has had episodes, definitive treatment is the way forward.
The definitive treatment is catheter ablation. Ablation is a procedure that takes the small area holding the extra pathway out of action by delivering energy to it. A thin catheter, a slim tube that delivers heat from its tip, is passed through a vein up to the heart. Once the location of the extra pathway is found, a short burst of energy is applied and the pathway is closed off. Ablation in WPW has a very high success rate. One session is usually enough, and the condition is resolved for good.
For patients who cannot have ablation or choose not to, rhythm medications can be used. These reduce how often episodes happen but do not remove the extra pathway. This is why ablation is offered first whenever it is suitable.
There are also a few moves a patient can try during an episode. Splashing the face with cold water, taking a deep breath and holding it, or bearing down firmly can sometimes stop the episode. The doctor teaches these moves and tailors the advice to the patient.
Sports and daily life
A common question is whether someone with WPW can do sports. The answer depends on the person. Those at low risk and without symptoms can usually take part in sports. For people thought to be at higher risk or with a history of episodes, ablation is offered first. After a successful ablation, the person can return to any kind of sport.
Professional athletes found to have WPW during screening are looked at in detail before being cleared. This is a precaution to prevent problems on the field.
WPW in children
Children can have WPW too. Sometimes it is found in infancy, sometimes only when an older child describes a racing heart. The treatment approach is similar to adults, but the choice to do an ablation depends on the child’s age, weight, and how often episodes happen. In very young children, the team often waits if possible and uses medication if needed. Once the child reaches a certain age and weight, ablation can be done safely.
When to call the doctor
A person already known to have WPW should reach out without delay if a long-lasting fast heartbeat starts suddenly, or if dizziness, fainting, or chest pain shows up. Episodes that come more often, last longer, or feel stronger also call for review.
A person who has had an ablation and starts feeling palpitations again months or years later also needs to be checked. In a small number of patients, the extra pathway may not have been fully closed, and a second procedure may be needed.
Frequently Asked Questions
Does WPW run in families?
In most cases there is no other family member with the condition. So most cases are not inherited. A very small group of families do see WPW in more than one member. For this reason, first-degree relatives with similar complaints should be checked.
What should I do during an episode?
First, try to stay calm and sit down. Splashing your face with cold water, taking a deep breath and holding it for a few seconds, or bearing down gently can stop the episode. If it does not pass within a few minutes, or if dizziness or near-fainting come along with it, go to the emergency room.
Will ablation get rid of the condition for good?
For most patients, yes. Once the extra pathway is closed, the racing episodes stop. In a very small number, the pathway is not fully closed or starts conducting again over time. A second procedure can be done in that case.
Can medication cure this condition?
Medication reduces how often episodes happen but does not remove the extra pathway. So medication is not a permanent fix. Ablation is the lasting solution.
Can a woman with WPW get pregnant?
Yes. Many women go through pregnancy with WPW without trouble. Still, since the heart works harder during pregnancy, episodes can become more frequent. For a patient planning a pregnancy, ablation before conceiving is often offered.
Does stress trigger episodes?
Stress, caffeine, alcohol, and lack of sleep can trigger episodes. They are not the cause of the condition, but they can help the already present extra pathway kick in.
My child has WPW. Can I sign them up for sports?
That call depends on the assessment. Children at low risk and without symptoms can take part in most sports. For those seen as higher risk or who have had episodes, treatment is planned first.